| Home | : | Biography | : | Fellowships & Awards | : | Publications | : | : | Mediation | : | Useful Links | : | Contact |
|
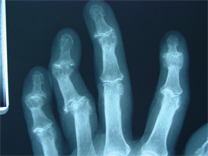
Finger Osteoarthritis Osteoarthritis is generally regarded as a condition of wear and tear. However there is certainly a genetic element to it. If a patient is going to develop arthritis it tends to occur in the hand first. The end joints of the fingers (distal interphalangeal joints DIPJ) are the most common joints in the body to get arthritis. The second most common joint in the body is the base of the thumb joint (carpometacarpal joint CMCJ). The most common complaints are joint stiffness, pain or deformity. X-rays are generally taken which show narrowing of the joint space, enlargement of the bone ends (osteophytes), cyst formation and bone sclerosis (whitening seen on the X-rays). Although each type of arthritis will be dealt with separately, generally the principles of treatment are:
Finger arthritis The finger has three joints, the end knuckle which is called the distal interphalangeal joint, the middle knuckle which is called the proximal interphalangeal joint PIP, and the knuckle nearest the carpometacarpal joint CMCJ. The distal interphalangeal joint
Treatment
After the surgery for DIPJ arthritis. The metacarpophalangeal joint is the first knuckle of the finger and is less commonly affected by arthritis than the DIPJ. It is probably less likely to be involved than the PIPJ. However it is affected fairly commonly again in women and the joints that tend to be affected are the joints of the index and middle finger.
Clinical features These are similar to arthritis anywhere else in the hand but essentially pain and stiffness can make the joints appear more swollen but they don't tend to get an angular deformity as in the PIPJ's and DIPJ's. Treatment Conservative (non-operative) This treatment is always started first: 1. Simple painkillers such as Paracetamol which has been proven to be a very effective painkiller (if you look at how a pharmacist determines how effective a drug is it is determined by the numbers of patients that the treatment is effective on and Paracetamol has a very high rating on this NNT grade). 2. Non-steroidal anti-inflammatory (NSAID's) drugs are specifically to reduce inflammation and although the NNT grade is not as great as Paracetamol these can be very effective and are the second line of treatment. The common ones used are Ibuprofen, Diclofenac or Eterocoxib. These are effective but have side affects as most pills and the side affects are stomach ulceration so any signs of heart burn or reflux indicate that these pills should be stopped. The Eterocoxib or Arcoxia has a stomach protective action which is beneficial for people who have difficulty taking non-steroidal anti-inflammatories. 3. Steroid injections - Once the Paracetamol and NSAID's options have become ineffective the next form of conservative treatment is to inject the carpo-metacarpal joint itself with some form of steroid. The most effective form of steroid is Triamcinolone which of the injected steroids has the longest action and is the most affective. It is generally mixed with a local anaesthetic in the form of Lignocaine or a longer acting anaesthetic such as Marcain. This injection can be carried out in the clinic and doesn't need to be done under X-ray control. However sometimes it is not feasible to get the needle into the joint and it may be necessary to use X-ray control. The injection is put in at the base of the thumb and can be painful. The steroid takes about 2 weeks to work and is not immediately effective and relief can last for 3 - 6 months. It is feasible to give two or three of these injections but there is a law of diminishing returns. The first works well, second less well and third is even less effective. It is Mr Field's practice to only give two injections. There are reasons for not injecting more than twice and that is the fact that steroid itself is damaging itself to articular cartilage and one may say so why is it done and the answer is that the cartilage in the joint is damaged anyway and you are really treating the symptoms and the symptoms only. MCPJ (first knuckle of the finger) replacement Joint replacements in the hand are generally performed for arthritis. It may be that in the future they are performed for unfixable fractures but at the moment that is not the case. Arthritis in the MCPJ's which is the first knuckle of the finger involves pain, stiffness and sometimes deformity. Pain, stiffness and deformity can all be corrected by joint replacement. The big advantage of joint replacement over joint fusion is that some movement will be maintained. It is important that the operation is not carried out to increase range of movement it may do so but, not necessarily. There are 10 year results for the MCPJ and there is 85 - 87% survival rate of these prosthesis.
|
|